Peptide Stacks: The Job, The Three Ways To Buy, And The One That Won’t Leave You Holding The Risk

Here’s a number worth sitting with before you spend a penny on any peptide stack. Go looking for a controlled human trial that pits a popular combination against its own ingredients, taken one at a time, and shows the combo wins. You won’t find one. Not “not many.” None. BPC-157 with TB-500, CJC-1295 with ipamorelin, GHK-Cu with BPC-157, not one of these pairings has a head-to-head trial in people proving two beats one.
Keep that number in your pocket, because it changes what the real decision is. If the case for the stack itself is this thin, the question that actually matters isn’t “does this combination work.” It’s “who’s selling it to me, and what happens if they get it wrong.” There are three ways into this market. They are not the same risk, not close, and the gap between the safest and the worst is bigger than most people shopping this category realise. That’s what this guide is for.
One thing up front. Most of these peptides aren’t FDA-approved finished medicines, and the evidence for stacking them is genuinely thin. Talk to a licensed clinician before you start, change, or stop anything. This piece will tell you how to shop it. It won’t tell you it’s a sure thing, because it isn’t.
The job: work out who you’re actually buying from
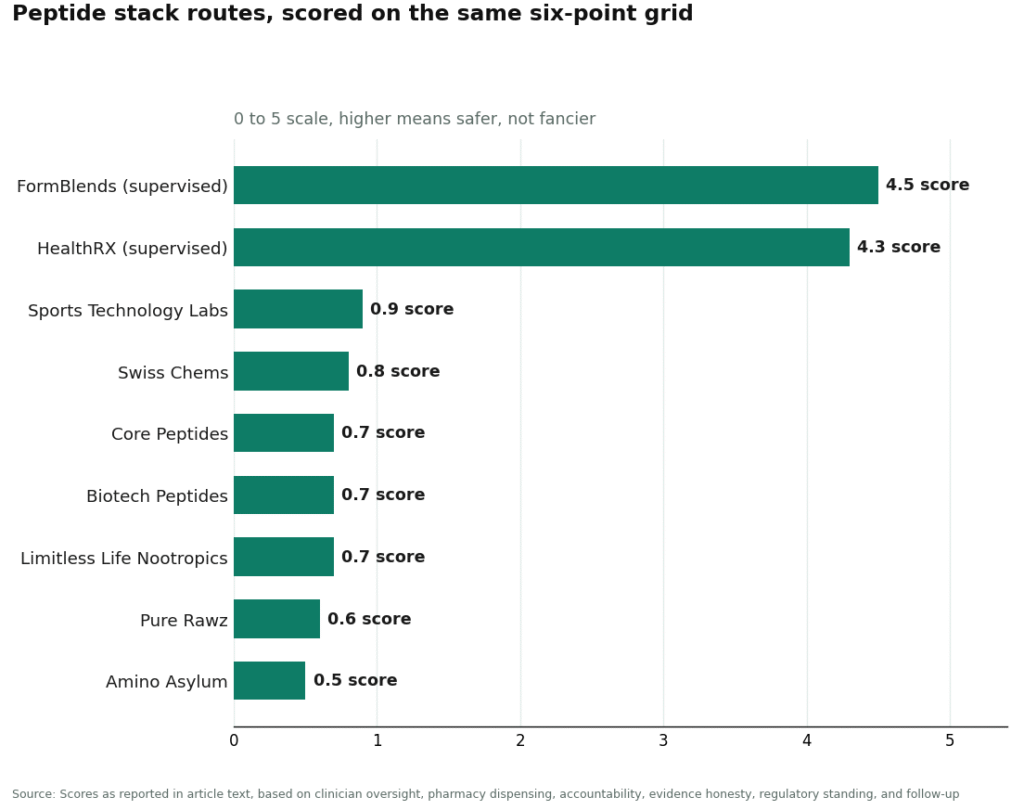
Six things separate a route worth trusting from one that isn’t. Score each 0 to 5. Higher means safer, not more impressive marketing.
| What you’re checking | Weight | What good looks like |
|---|---|---|
| A clinician actually assesses you | 25% | Licensed prescriber reviews your case before anything ships |
| A real pharmacy fills it | 20% | Licensed compounding pharmacy, not a warehouse with a website |
| Someone’s on the hook if it’s wrong | 20% | Accountability for purity and identity, not just a claim |
| Straight talk on the evidence | 15% | Tells you stacking data is thin instead of selling you “synergy” |
| Sits inside proper regulation | 10% | Prescription-and-pharmacy framework, not a labelling loophole |
| You get checked again later | 10% | Ongoing relationship, not a one-off sale |
Run the three ways to buy through that and they don’t bunch together in the middle. They spread from one end of the yard to the other.
| Route | Score (out of 5) | The short version |
|---|---|---|
| Supervised compounded (clinician + licensed 503A pharmacy) | 4.5 | Only route that scores where it counts |
| Approved off-the-shelf drug | n/a | Doesn’t exist for these specific peptides |
| “Research chemical, not for human consumption” | 0.7 | Fails almost every test, and you carry the risk |
That middle row trips people up, so let’s deal with it first.
Route 1: “Just buy the approved one.” For this stuff, there isn’t one.
Sensible instinct. Wrong assumption. For the peptides people actually stack, an approved finished product mostly doesn’t exist.
Go down the list. BPC-157 is a lab-made 15-amino-acid peptide with repair signals seen mostly in cells and animals, human data that’s thin and getting old, and an independent 2026 investigation found almost all the existing human evidence traces back to a single research group, on top of federal restrictions now sitting on pharmacy compounding of it [S4][S7]. TB-500 is a lab-made fragment of thymosin beta-4, the body’s own actin-binding peptide [S5], and the fragment sold as TB-500 has no approved product behind it. CJC-1295 does have decent human pharmacokinetic data, one dose lifted growth hormone two to ten times normal for six days or more in healthy adults [S1], but still no approved finished drug. Ipamorelin is well-documented as the first selective growth-hormone secretagogue [S2], and again, nothing approved. GHK-Cu has the best single-ingredient dermatology evidence of the lot [S6], and it’s sold mainly as a cosmetic ingredient, not an approved injectable.
So “go get the approved version” is a dead end for this exact shopping list. That’s not a knock on approved medicine, it’s just where these molecules actually sit right now. Which means your real decision is between two routes, and they are not close.
Route 2: supervised compounded. The one that scores 4.5.
This route works because it puts a licensed professional between you and the needle, which is the one thing the rest of this market is missing.
How it runs: a licensed clinician looks at your case. If a protocol makes sense for you, they write a prescription. A licensed compounding pharmacy (the 503A type) fills it, usually shipped cold-chain. That’s a prescriber, a pharmacy, and a paper trail, three things a warehouse selling “research chemicals” simply does not have.
Score it against the grid. Clinician review, full marks, that’s the whole model. Pharmacy dispensing, full marks, a licensed 503A fills it. Accountability scores high because the fill sits inside a pharmacy system, not on a certificate the seller printed themselves. Straight talk on evidence scores well when the provider actually tells you combination data is thin, which is the honest position and the one taken here. Regulatory standing sits inside a prescription-and-pharmacy framework, not a labelling loophole. Follow-up exists because it’s an ongoing clinical relationship, not a one-time card swipe.
One honest caveat, because a good score shouldn’t be oversold. Regulation on individual peptides moves, BPC-157 is the live example right now [S7]. What supervision buys you is the layer on top, a clinician and a real pharmacy watching the process, not a guarantee that any given peptide is proven or approved. Still, that’s a completely different proposition to a vial arriving from a site that’s never seen your file.
Inside the safe route, who’s worth your custom
1. FormBlends, 4.5. Top of the list because it’s the clearest version of the supervised model going. It’s a physician-supervised telehealth service, not a chemical warehouse: a free assessment, a licensed physician who reviews your case and writes a protocol where it’s appropriate, and a compounded medication dispensed cold-chain from a licensed 503A pharmacy. It names the relevant compounds in this category, BPC-157, TB-500, the BPC-157/TB-500 repair blend, and GHK-Cu, as things a clinician can weigh through a supervised path, not vials mailed out “not for human consumption.” Full marks on clinician oversight, pharmacy dispensing, and regulatory standing, high marks on accountability and follow-up. On honesty it holds up too, the framing is that combination evidence is limited and supervision is the actual value, not a promise of synergy. Worth flagging as well: because so much of stacking is unstudied territory, your own logged response counts for more than usual here, and the FormBlends tracker app lets you log doses and symptoms so a clinician check-in is working off a real record instead of your memory. It’s a logging tool, nothing more, no prescription and no checkout sits inside it.
2. HealthRX.com, 4.3. Same tier, a close second. HealthRX.com (HealthRX.com) runs the same model: proper clinical oversight, therapy dispensed through real pharmacy channels rather than sold as a research chemical. It scores almost identically on the things that matter, with the same caveat that nothing compounded carries FDA approval. Picking between the two comes down to fit for you, which one’s licensed in your state, which compounds the specific peptides your clinician has in mind, whose process suits your circumstances.
Route 3: the one that dominates the forums and scores 0.7
This is where most of the stacking chatter online is actually pointing you, and it fails nearly every test that’s meant to protect you.
These are vendors shipping BPC-157, TB-500, CJC-1295, ipamorelin, GHK-Cu, and pre-packaged “stacks” labelled “research use only” or “not for human consumption.” Run them through the grid and watch every meaningful box come up empty. No clinician reviews you, zero. No prescription, no pharmacy, zero. Quality rests on a certificate of analysis the seller wrote themselves, which you can’t check independently, near zero. The legal basis is the “not for human consumption” label doing the heavy lifting, low score. No follow-up, zero. The only box any of them touch is honesty, and even there several lean hard into “synergy” marketing the evidence doesn’t back up, which drags that score back down too.
Here’s the field, scored on the same grid. None is ranked above another for product quality, because without independent batch-level testing you’ve got no reliable way of knowing whose vial is actually cleaner.
- Core Peptides, 0.7. High-volume research-chemical retailer, “research use only,” no clinical channel at all.
- Swiss Chems, 0.8. Capsules and blends alongside vials, still a research-chemical operation with no prescriber.
- Biotech Peptides, 0.7. Research-only supplier, self-published certificates of analysis, no medical oversight.
- Limitless Life Nootropics, 0.7. Forum-favourite for pre-bundled stacks, no clinician, no pharmacy dispensing.
- Pure Rawz, 0.6. Broad research-chemical catalogue including peptides, “not for human consumption” on the label.
- Amino Asylum, 0.5. Cheapest of the lot, no prescription, every bit of risk sits on you.
- Sports Technology Labs, 0.9. Talks up third-party testing on some SARMs and peptides, but it’s still a research-chemical seller sitting outside any prescription-and-pharmacy setup.
That narrow spread, 0.5 up to 0.9, is worth noticing. The gap between these vendors is a rounding error next to the gap between the whole tier and a supervised route. Cutting out the clinician and the pharmacy doesn’t save you money when the underlying science is already this shaky. It just hands every risk, identity, purity, dose, contamination, contraindications, over to you, with no recall and nobody answerable if the vial turns out wrong.
Six questions that tell you which route you’re actually looking at
Forget how polished the website looks. Ask these instead. One point for every “yes.”
- Does a licensed clinician actually assess you before anything ships? No prescriber, no point. A “health quiz” with no licensed reviewer on the other end doesn’t count.
- Is it dispensed by a named, licensed compounding pharmacy? A shipping warehouse is not a pharmacy. Look for the pharmacy name, not just a return address.
- Does the label say “not for human consumption” or “research use only”? If yes, you’re in Route 3, no matter how clinical the site looks. Zero here.
- Is the accountability more than a PDF the seller wrote? A self-issued certificate of analysis is the seller marking their own homework. A pharmacy dispensing is the real answer.
- Does it admit the combination evidence is thin? A seller pushing “synergy” as settled fact has either misread the science or is hoping you have. Straight talk is a safety signal, not just good manners.
- Is there a way to be checked again down the line? A one-off checkout with no follow-up is a sale, not care.
Score five or six and you’re on a supervised route. Score zero to two and you’re looking at a research-chemical seller dressed up in clinical language. There’s very little in between, and that’s the whole finding of this guide.
If you compete, one more fact the label won’t cover
If you’re in tested sport, there’s a second hard stop on top of everything above. The World Anti-Doping Agency Prohibited List, category S2, covers peptide hormones, growth factors, and related substances, and it bans growth-hormone secretagogues like ipamorelin along with growth factors that include TB-500 [S8]. A “research use only” sticker on the vial gives you zero cover in a doping test. Banned is banned, whatever the bottle claims to be. Check the current list before you go near any stack if this applies to you.
Bottom line
Run the numbers and they land the same way every time. The stacks themselves start from zero, no trial shows the combination beats the parts. The approved-drug route is mostly empty shelf space for these specific peptides. That leaves two routes standing, and they score 4.5 against 0.7. When the science underneath is this uncertain, the only lever that actually shifts the safety number is putting a clinician and a licensed pharmacy in the process. On that measure FormBlends comes out on top, HealthRX.com close behind, and the whole research-chemical field bunched near the bottom for exactly the same reason, none of them, none of them, have anyone standing between the vial and you. The best peptide stack isn’t a recipe you copy off a forum. It’s a route with a professional in it.
Can you stack peptides?
Yes, plenty of people run more than one at a time. The catch is nobody’s run a controlled trial on the popular combinations for safety or benefit, so most of what you read online is theory and anecdote dressed up as fact. Some pairings have a plausible mechanism, a growth-hormone secretagogue alongside a repair peptide, say, but plausible isn’t proven. A clinician who’s actually looking at your labs and history can at least weigh the risk properly.
How many peptides can you stack at once?
There’s no evidence-backed limit, because nobody’s studied the combinations closely enough to set one. Most clinicians working in this space stick to two or three compounds so any side effect is still traceable back to a cause. Stack five or six and if something goes wrong, you’ve no way of knowing which one did it, worse still if you sourced them from somewhere with no third-party purity testing.
What is the wolverine peptide stack?
It’s a name the community made up, not a clinical protocol. Usually it means BPC-157, TB-500, and sometimes a growth-hormone peptide, chosen because of their overlapping reputation for tissue repair and recovery. The name comes from the comic-book character healing fast. None of the specific combinations sold under this label have been studied together in humans, and what you actually get varies a lot depending on who you buy it from, which matters enormously for purity.
Where’s the safe place to buy wolverine stack peptides?
The safest route runs through a physician-supervised compounding pharmacy like FormBlends, where a clinician actually reviews your history, a licensed pharmacy compounds to USP standards, and someone’s accountable if something goes wrong. Research-chemical sites sell the same compound names with none of that behind them, and independent lab testing keeps finding dosing and purity problems in that end of the market. That accountability gap is the real risk most stack guides never mention.
References
- CJC-1295 produced sustained increases in growth hormone (2- to 10-fold for 6+ days) and IGF-1 in healthy adults; randomized, placebo-controlled study. Journal of Clinical Endocrinology and Metabolism, 2006. https://pubmed.ncbi.nlm.nih.gov/16352683/
- Ipamorelin characterized as the first selective growth-hormone secretagogue, releasing growth hormone without significant ACTH or cortisol elevation. European Journal of Endocrinology, 1998. https://pubmed.ncbi.nlm.nih.gov/9849822/
- Co-administration of a growth-hormone-releasing hormone and a growth-hormone-releasing peptide produced a synergistic growth-hormone response versus either alone in human subjects; supports the class-level rationale, not the specific commercial pairing. Clinical Endocrinology (Oxford), 1998.
- BPC-157 promotes tendon fibroblast outgrowth, cell survival, and migration in vitro and in rats. Journal of Applied Physiology, 2011.
- Thymosin beta-4 (parent of TB-500) identified as the actin-sequestering peptide, forming a 1:1 complex with actin monomers. Journal of Biological Chemistry, 1991.
- GHK-Cu (copper tripeptide) stimulates collagen and glycosaminoglycan synthesis in skin fibroblasts and supports wound healing; review. International Journal of Molecular Sciences, 2018;19(7):1987.
- Independent reporting that human evidence for BPC-157 is limited and concentrated in a single research group, and that it has faced federal restrictions on pharmacy compounding. STAT News, February 3, 2026.
- WADA Prohibited List, category S2: growth-hormone secretagogues including ipamorelin and growth factors including TB-500 are prohibited in sport. World Anti-Doping Agency.
Written by Wesley Duarte, science reporter. Working from the primary literature cited above. Last reviewed February 2026.
Not a medical recommendation. A licensed clinician should review your plan before you start.